A 70 year old female with constipation, Anemia, post prandial pain abdomen
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs". This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome.









 ECG
ECG

I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
This is a case of a 70 year old female admitted in the ward, with a history of
low grade fever
loss of appetite
constipation.
History of presenting illness
She presented with a 15 day history of early satiety and post prandial pain. i.e, she eats at 1:00 pm; develops pain at around 3-4 pm in afternoon in left hypochondrium region burning type non radiating, which is gradually progressive and severe by around 3-4pm , vomits (induced) at around 6 pm). The vomiting is non bilious non blood stained non foul smelling food as content.
She also complains of occasional occurence of streaks of blood in stools which probably is more likely to be because of anal fissure due to constipation
She was diagnosed as having a duodenal ulcer. And due to severe Anemia she was given blood transfusion.
In the year 2020, history of Endometrial carcinoma for which she was treated with Chemotherapy and radiotherapy in MNJ for 1 and a half month.
3 years ago, she fell from an auto, while sitting at the back in a 7 seater and slipped and fell when the auto sped over a speedbreaker. She had a femur fracture which was operated on (proximal femoral nail). She denies having lost consciousness at that time. No h/o trauma to head and other injuries.
She also reports dizziness and transient blackouts while she brushes her teeth after she gets up from the bed.
Past history-
She was diagnosed with hypertension 10 years ago and is on regular medications.
No h/o DM Bronchial asthma CAD TB COPD
No h/o past surgeries (except for femur nail implant)
Personal history-
Diet- mixed
Appetite- decreased
Sleep- adequate
Bowel (constipated) and bladder regular
No Addictions
Family history
Not significant
Allergic history
No known allergies
General physical examination-
Vitals - PR - 76 BPM
BP - 170/80 mm Hg
RR - 16/min
Temp - 100.6°F
Temporal wasting, deltoid wasting, increased skinfold thickness at triceps, mild proximal myopathy
Pallor ++
No icterus cyanosis clubbing lymphadenopathy pedal edema
Pale tongue
Hyperpigmented lesions on tongue
Maculopapular lesions on lower chest and upper abdomen
Pedal edema
Pitting type grade 2
(edema resolving over several minutes)
CVS -
Inspection-
Shape of chest- elliptical
No scars dilated veins
No raised JVP
Apical impulse visible and appeared to be heaving.
Palpation-
Apex beat felt in left 6th ICS MCL more laterally
Parasternal heave+
Collapsing water hammer pulse + (felt in carotids)
No radio radial delay.
No thrills,
Auscultation-
An ejection systolic murmur in the aortic area without Gallavardin phenomenon. S3 heard in mitral area.
GIT examination-
Inspection
Shape of abdomen- scaphoid
No scars sinuses visible pulsations dilated veins abdominal distension
All quadrants moving with respiration
Umbilicus everted
On palpation
No tenderness
No local rise of temperature
Soft abdomen, no organomegaly
Percussion
Liver dullness in 5th ICS
Splenic dull note in 8th ICS MAL (mild splenomegaly)
Auscultation
Bowel sounds heard
CNS -
Higher mental functions- intact
Cranial nerves intact
Sensory- fine touch, crude touch, pressure, temperature, vibration senses intact.
Motor system
Power: 5/5 in both UL and LL
Tone- normal
Bulk - decreased
Reflexes:
Biceps, Triceps Supinator Knee reflexes intact (++)
No cerebellar signs noticed
Respiratory system -
Shape of chest elliptical
B/l symmetrical expansion of chest wall+
Position of trachea- central
Resonance present in all lung fields
BAE+ NVBS+
No crepitations heard
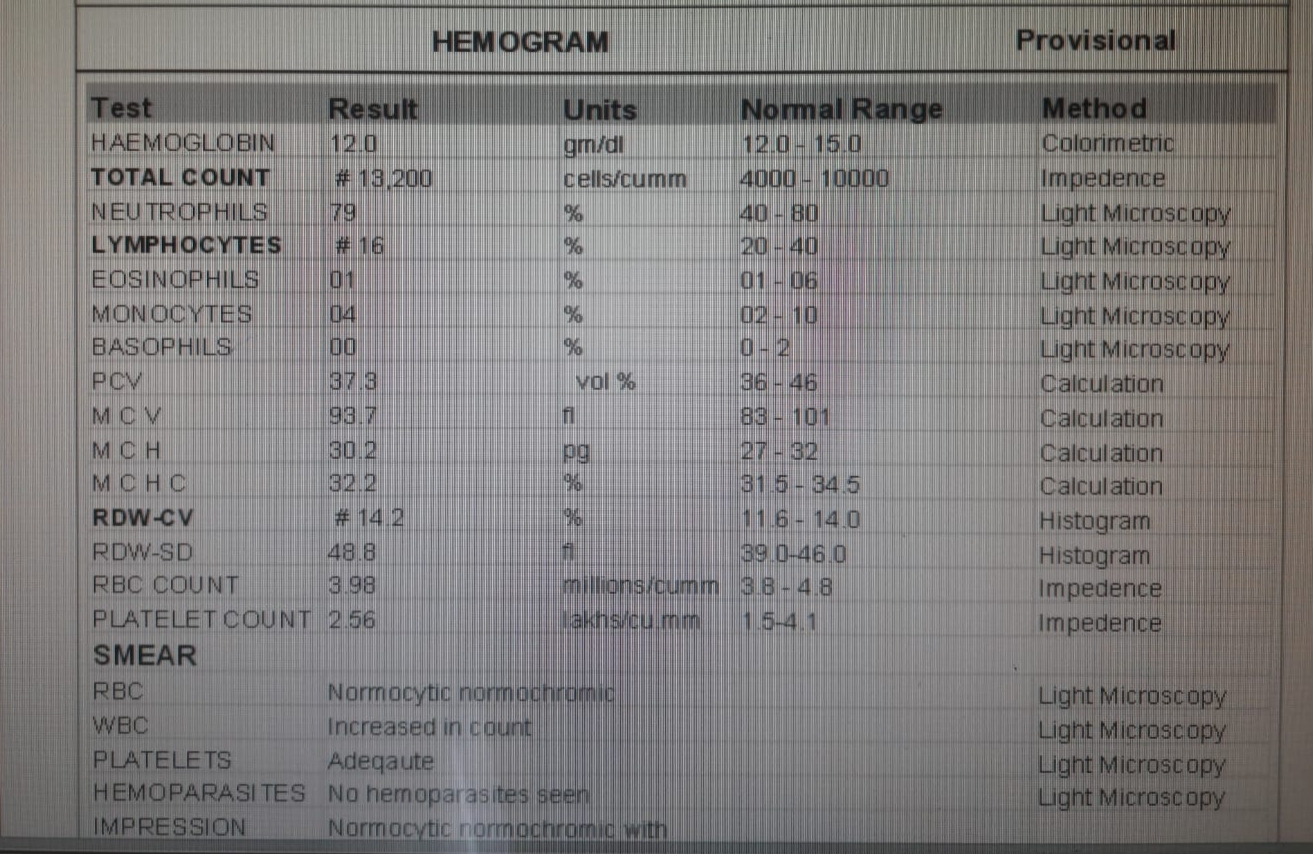
Hemogram- Severe anemia ; Hb 4.3
Iron studies- serum ferritin at 3.9 ng/ml - iron deficiency
Hypoalbuminemia at 3.2g/dl. Creatinine at 1.5mg/dl with eGFR at 40 ml/min/1.73m2
CXR -
Showing left ventricular hypertrophy with unfolding of aorta
USG abdomen-
Revealed- mild ascites
Right renal cal
Renal cortical cysts
2D Echo -
Moderate to Severe AR
Moderate to Severe AS
AS (thickened calcific) + AR + Concentric LVH (IVS at 1.5cm, and HTN since only 4 years which is usually well controlled)
Diagnosis -
Metastatic carcinoma?
Amyloidosis?
Pernicious Anemia


Comments
Post a Comment