56 YEAR OLD MALE WITH ABDOMINAL PAIN AND OLIGURIA
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.




















Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment box is welcome.
A 56 year old male agricultural labourer by occupation, resident of Muthagudem came to OPD on 13/01/22 with the chief complaints of-
Pain abdomen since 20 days
Vomitings since 20 days
Fever since 15 days
Decreased urine output since 15 days
Patient was apparently asymptomatic 3 years ago and then he developed
B/l loin pain which was sudden in onset gradually progressive and associated with high grade fever.
1 year ago he developed pedal edema upto ankle, decreased urine output, burning micturition, flank pain which is dragging type, radiating towards abdomen, but the patient did not get himself checked due to financial issues.
3 months ago they visited nalgonda hospital with the same complaints there he was diagnosed with b/l renal calculi. He was given medication after which it got resolved.
After 2 months he again had developed decreased urine output and b/l pedal edema on and off. Since then he stopped going to work.
On 02/01/22
He went to a hospital in Nalgonda with C/O fever with chills and rigors and generalised body pains for 3 days
USG report showed
Right gross pyonephrosis
Left gross hydronephrosis
Liver hemangioma
For which he was given medication and referred to urologist.
On 08/01/22
He was taken to a hospital in khammam where his
USG -
Serum Creatinine - 11.2 mg/dl
On 12/01/22
He was taken to another hospital in Nalgonda with c/o
b/l loin pain, fever, vomiting, dysuria and reduced urine output.
On CT abd:
Gross HDN of Rt kidney with proximal ureteric calculus of 2 cm.
Lt severe HDN with 2.6 cm mid ureteric calculus
Right kidney and ureter-
Left kidney and ureter-
Patient was counselled about requirement of haemodialysis and was referred to KIMS Narketpally
He underwent a session of dialysis on 15/01/22
Past history-
Not a k/c/o HTN, DM, TB, Asthma, epilepsy.
Personal history-
Diet - mixed
Appetite- reduced
Sleep - reduced
Alcoholic since 10 years takes 90 ml everyday
On general physical examination
Patient is conscious coherent and cooperative
Thin built and malnourished
Pallor+ clubbing+
No icterus, cyanosis, lymphadenopathy
Vitals on 13/1/22
Temp- afebrile
BP- 140/80 mm hg
PR- 100 bpm
RR- 22 bpm
Spo2- 98 % at RA
GRBS- 116 mg/dl
On systemic examination-
CVS- S1 S2 + No murmurs
RS- BAE+ No added sounds
P/A- soft, tender, bilaterally symmetrical, no organomegaly
CNS- No focal neurological deficits
Investigations-
RFT:
Urea- 278
Creat- 16
Na-134
K-6.1
Cl-104
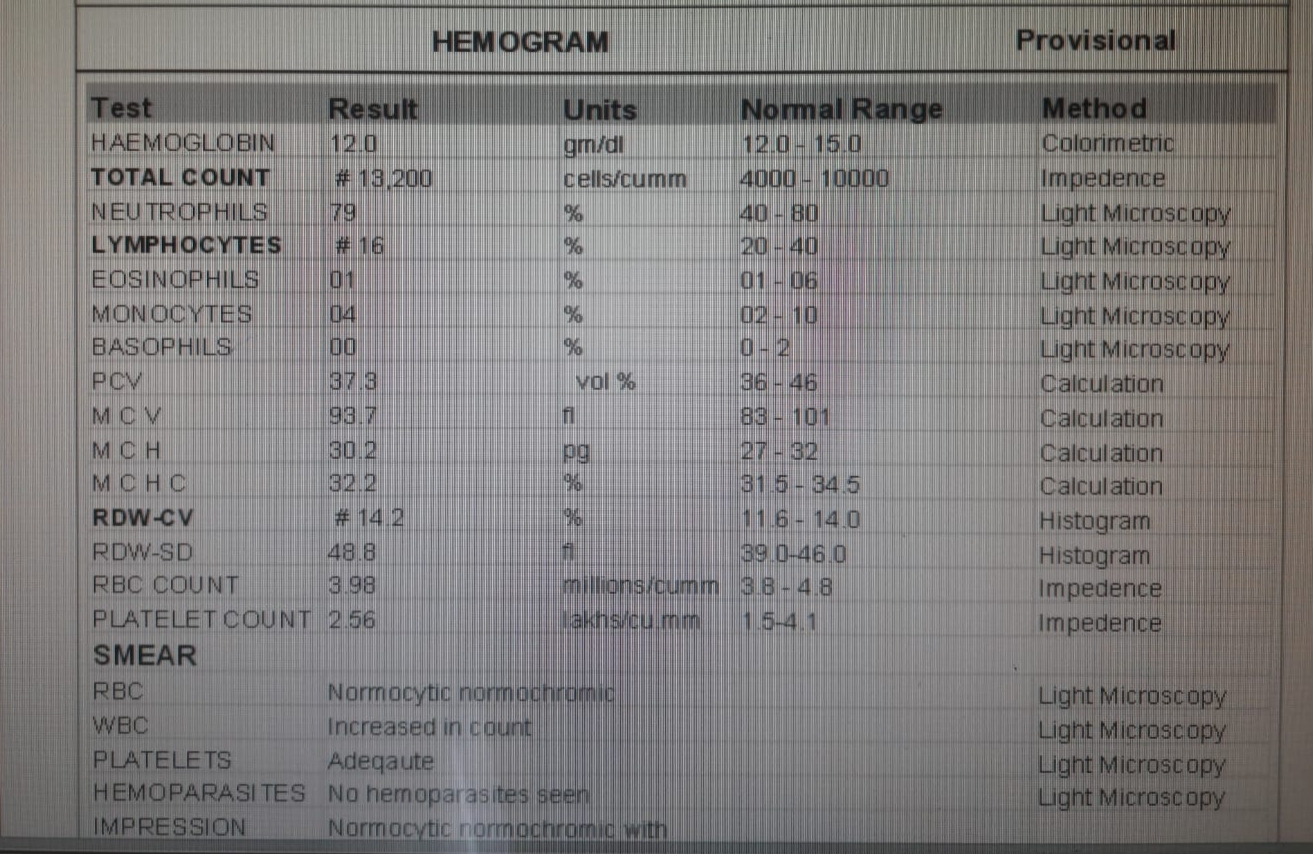
Hemogram:
Hb-7.9
TC- 6,400
PLC- 2,40,000
CUE
Alb- 1+
PC- 3-4
LFT:
TB- 0.99
DB- 0.28
AST-12
ALT-12
ALP- 174
TP-6.4
Alb-5.5
ABG:
PH- 7.21
Po2- 131
Pco2-14.5
Spo2-96
HCo3-5.7
ECG-
On the day of admission
Diagnosis:
Post renal AKI secondary to b/l hydronephrosis with refractory hyperkalemia (secondary to renal calculus) with metabolic acidosis
Treatment:
Inj HAI 10 IU in 25%D slow IV/ stat over 30 mins to 1 hour
Inj calcium gluconate 10 ml slow IV a/r 10 mins
Inj Thiamine 1 amp in 10 ml NS IV over 30 mins/ OD
Inj Sodium bicarbonate 50 meq IV/ stat slowly over 10-20 mins
Nebulisation with duolin
IV fluids
Inj lasix 20 mg IV/BD
Inj Zofer 4 mg IV/TID
Tab Orofer XT PO/OD
Tab Nodosis 500 mg PO/BD
Inj Pan 40 mg IV/OD
Tab PCM 650 mg PO/SOS
Salt restriction < 2.4 g/ day
On 19/01/22
LEFT PERCUTANEOUS NEPHROSTOMY UNDER LOCAL ANAESTHESIA IS DONE
One session of haemodialysis done on 19/1/22
C/o fever with chills , 1 g neomol given.
X ray kidney ureter bladder-
On 20/01/22
SOB reduced
Fever spikes present 104 F
Cough reduced
O/E -
Patient is c/c/c
Febrile 102.6 F
BP - 100/70
PR - 88bpm
CVS - S1S2+
RS - BAE+
P/A - soft, non tender
Creatinine : 16.3 --> 9.5
Urea : 278 --> 162 --> 217
USG abdomen-
Findings:
Grade II RPD changes in Lt kidney
Grossly dilated PCS of Rt kidney compressing the renal parenchyma.
Plan -
To watch for reduction of urea and creatinine


Comments
Post a Comment