A 17 year old girl with mucosal hyperpigmentation and hypothyroidism
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs". This E log book also reflects my patient-centred online learning portfolio and your valuable comments on comment box is welcome.








 ACANTHOSIS NIGRICANS OVER NECK-
ACANTHOSIS NIGRICANS OVER NECK-












I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
A 17 year old female; student; resident of Mothkur, presented with the chief complaints of :
Vomitings since one week
Loose stools since one week
History of presenting illness:
Patient was apparently alright 10 years ago then her mother noticed a swelling in the anterior aspect of patient's neck which was painless and was gradually increasing in size. She was taken to hospital where she was diagnosed to have HYPOTHYROIDISM and was started on tab. Thyroxine sod. 25mcg
She developed PICA since 3 years (had been eating chalks and slate pencils). She also has a habit of leg shaking.( Restless leg Syndrome?)
She also complains of AMENORRHEA since 3 months (since August) .
Age of menarche - 11 years
30 day cycle, regular, menses for 4-5 days, changes 4 pads per day, not a/w pain abdomen , clots, burning micturition, discharge, change in voice, abnormal hair growth, hair loss.
LMP- 25/10/22. Associated with clots (2*2) cm
She is a known case of Anemia since 3 years and complains of SOB on exertion or climbing stairs (NYHA-ll) . She also complains of feeling DIZZY as soon as she gets up from the bed.
No h/o sweating, tremors, loss of consciousness, palpitations, headache, muscle pains.
She has a weight gain of nearly 20 kg from past 2-3 years., i e from 45 to 65 kgs.
She now complains of vomitings after food since one week which was sudden in onset, projectile, non bilious non blood stained, non foul smelling, food as content.. occuring 5× a day
Watery Diarrhea since one week, sudden in onset, non blood stained, non foul smelling, 4-5 times a day, associated with pain abdomen
Not a/w abdominal distension, constipation, purulent discharge in stools
Past history:
No h/o similar complaints in the past
K/c/o hypothyroidism since age of 7 years
No h/o DM, HTN, Bronchial asthma, CAD, TB, epilepsy.
No h/o blood transfusions
Personal history:
Diet- mixed diet
patient has been staying in hostel since 10 years
According to her dietary routine, she has deficit of milk and leafy vegetable consumption.
She complains of loss of appetite since one week
Sleep - adequate
Bowel and bladder movements- regular
No Addictions
Family history
Mother is a k/c/o hypothyroidism and on THYRONORM 100mcg
Drug history
She has been on thyroxine sod since 10 years.
Allergic history:
She had an allergy 3 years back for which she had rashes on her body and subsided on medication
General physical examination:
Patient is concious coherent and cooperative well oriented to time place and person
Well built and nourished
Height- 160 cm
Weight- 65kg
BMI- 25.4 (overweight)
Vitals
Temperature- afebrile
HR
BP
RR
GRBS
Pallor - present
Icterus, clubbing, cyanosis pedal edema - absent
Submandibular and cervical lymph nodes enlarged.
Tongue-
Pale smooth and shiny
Hyperpigmentation over knuckles and palmar creases present
O/E of oral cavity:
hyperpigmented patches were noticed on palate and mucosa of cheek on either side
Angular stomatitis, yellowish brown pigmentation over teeth noted.
Systemic examination-
GIT examination-
Inspection-
Shape of abdomen- scaphoid
No scars sinuses visible pulsations dilated veins abdominal distension
All quadrants moving with respiration
Umbilicus everted
On palpation-
No tenderness
No local rise of temperature
Soft abdomen, no organomegaly
On Percussion-
Liver dullness in 5th ICS
On auscultation-
Bowel sounds heard
CVS
Inspection-
Shape of chest- elliptical
No scars dilated veins
No raised JVP
Palpation-
Apex beat felt in left 5th ICS MCL
No thrills, parasternal heave felt
On auscultation-
S1 S2 heard, no murmurs
Respiratory system examination-
Shape of chest elliptical
B/l symmetrical expansion of chest wall+
Position of trachea- central
Resonance present in all lung fields
BAE+ NVBS+
No crepitations heard
CNS examination
Higher mental functions- intact
Cranial nerves intact
Sensory- fine touch, crude touch, pressure, temperature, vibration senses intact.
Motor system
Power: 5/5 in both UL and LL
Tone- normal
Bulk - normal
Reflexes:
Biceps, Triceps Supinator Knee reflexes intact (++)
Ankle reflex 5+
No cerebellar signs noticed
Local examination of thyroid
A diffuse swelling in anterior aspect of neck 7*8 cm approx was noticed, moves with deglutition, skin on swelling normal , no scars fistula seen
Non tender ,Smooth surface, firm in consistency, trachea central, carotid pulsations present.
No bruit on auscultation
Investigations-
Hemogram:
Sr. Iron
Peripheral smear
Dimorphic picture showing microcytic and macrocytic cells with pencil cells, elliptocytes, few tear drop cells
WBC normal morphology
Platelets increased
Sr. Calcium:
Thyroid function tests:
Sr. Ferritin
CXR
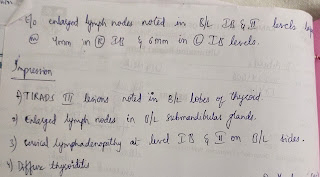
USG neck
USG of abdomen - no abnormalities detected
Uterus- polycystic morphology detected in both the ovaries
Cystitis seen
ECG :
In suspicion of Addison's
cosynaptin stimulation test was done.
Inj. ACTH was given on 4:30 pm on 2/11/22
Reports on 3/11/22:
Levels of sr.cortisol at 5:30 pm
Baseline cortisol levels at 8am:
Provisional diagnosis:
Pernicious Anemia with autoimmune thyroiditis
TREATMENT:
1.NALMOL
2.TAB.PANTOP 40mg BD
3.TAB.ZOFER 4mg SOS
4.TAB.SPOROLAC (ROUTE:PERORAL) BD
5.TAB.DOLO 650mg SOS
6.TAB.THYRONORM 25mcg OD
7.ORS SACHET IN 1LT WATER TO DRINK AFTER EACH LOOSE STOOLS.
8.VITALS STORING EVERY 4TH HRLY
Comments
Post a Comment